


The chemotherapy is often the part patients dread most. Before a person with sickle cell disease can receive gene therapy, doctors usually wipe out the blood-making cells in their bone marrow with a punishing dose of a drug called busulfan. It clears space for the corrected cells to take hold, but it also brings weeks of low blood counts, infection risk, hair loss, and a lasting hit to fertility. For a therapy meant to end a lifetime of pain, that opening act feels like a cruel toll.
A team led by researchers at Cincinnati Children's Hospital set out to see whether the toll could be smaller. In a phase 1/2 trial reported in Nature Medicine, they treated seven people with sickle cell disease using a milder conditioning regimen and their own genetically modified stem cells. The oldest results now stretch back seven years. Across that span, severe pain crises fell by more than 80 percent, and the patients avoided the worst of what standard conditioning usually inflicts.
Rewriting the blood at its source
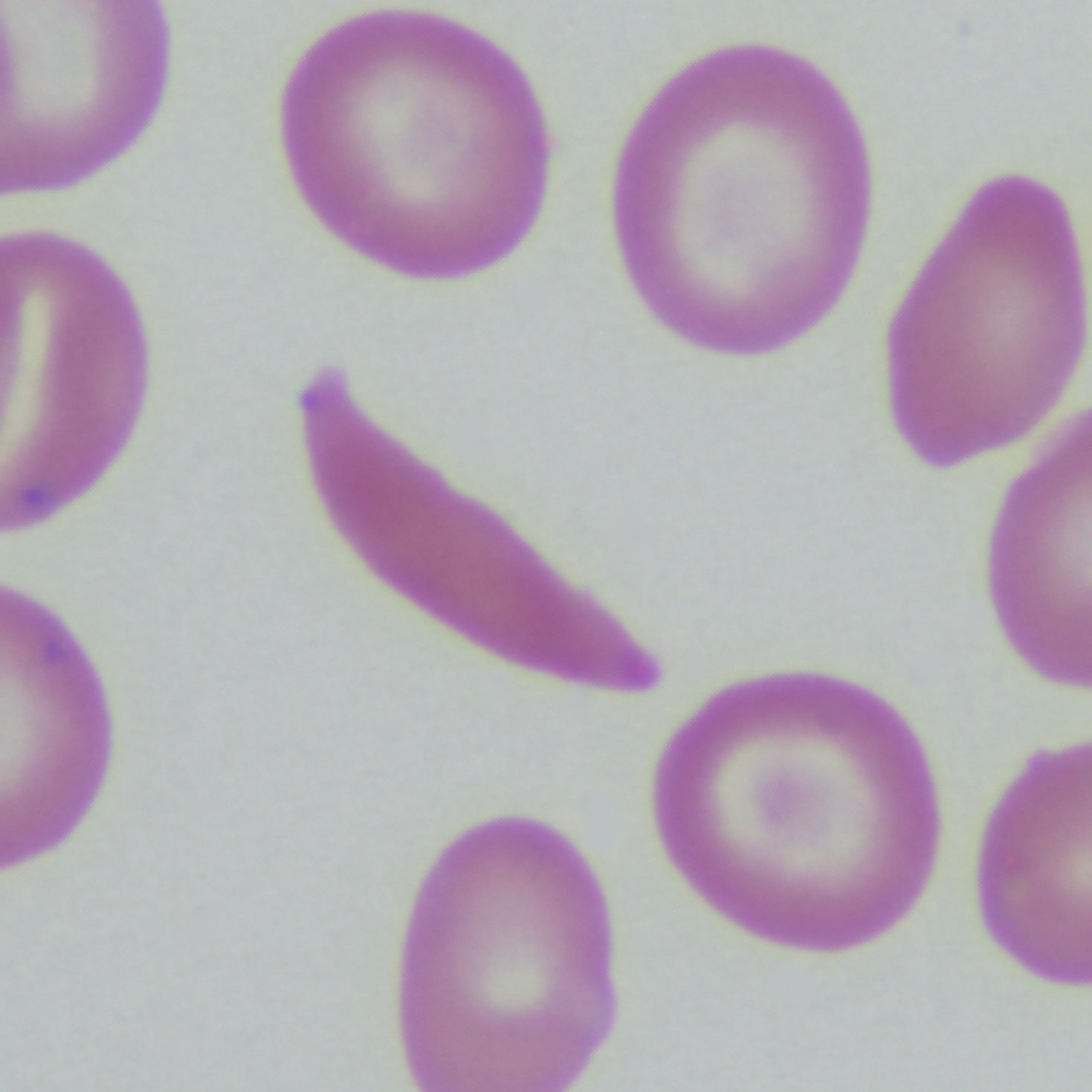
Sickle cell disease comes from a single typo in the gene for hemoglobin, the protein that carries oxygen in red blood cells. That one change makes the cells stiffen into a crescent shape under stress. The warped cells jam small blood vessels, starving tissue of oxygen and setting off the bouts of agony known as vaso-occlusive crises. Over years, the damage accumulates in the lungs, kidneys, and brain.
The approach here does not fix the broken gene directly. Instead, the researchers pulled hematopoietic stem cells, the cells that generate all blood, from each patient. In the lab, they used a lentiviral vector, a stripped-down virus repurposed as a delivery truck, to insert a modified version of the gamma-globin gene. That gene switches on fetal hemoglobin, the oxygen-carrying form we make before birth and normally shut off in infancy. Fetal hemoglobin resists sickling, so red cells built with it stay flexible. The engineered cells were then infused back into the patient after conditioning.
What set this trial apart was the dose of that conditioning. The team used reduced-intensity conditioning rather than the full myeloablative blast. The bet was that even a modest amount of gene-corrected marrow, if it produced enough fetal hemoglobin, could tip the balance away from disease without demanding a total marrow reset.
What the numbers showed
All seven patients produced sustained fetal hemoglobin from the added gene, and all saw a drop of more than 80 percent in severe vaso-occlusive events. The lighter conditioning did what the team hoped. The median stretch of the most severe low-platelet counts lasted about five days, and the deepest neutropenia, the shortage of infection-fighting white cells, ran about eight days. Those are short windows compared with the weeks that full conditioning can impose.
The safety record was not spotless, and the paper does not pretend otherwise. Across the seven patients over the full study, investigators logged 503 adverse events. The most common were grade 2 to 3 vaso-occlusive crises, the very problem the therapy targets, which can still flare in the period before the corrected cells fully take over. No new sickle-related organ catastrophes derailed the results, and the reduced conditioning appeared to spare patients the harshest toxicities of the standard version.
The trial was stopped after the seventh patient, not because it failed but because it had met its predefined goals and the industry funding had run out. In a field where many gene therapy programs quietly stall, hitting the endpoints and reporting years of follow-up counts as a real result.
What the study can't say yet
Seven patients is a small number. With no control group and an open design, it is impossible to know precisely how much of the benefit traces to the lighter conditioning versus the gene therapy itself, or how the milder regimen would stack up head-to-head against the full-dose approach. The trial was built to test safety and feasibility, and it answered those questions. It was never powered to prove that reduced-intensity conditioning is as durable as the standard.
There are open questions about the vector, too. Lentiviral gene therapies insert their cargo semi-randomly into the genome, and long-term monitoring for any cancer risk from that insertion remains essential. Seven years of clean follow-up is reassuring, but blood cancers can take longer to surface, so the watch continues.
Still, the direction matters. Approved sickle cell gene therapies already exist, and they work, but their reliance on heavy chemotherapy keeps them out of reach for many patients who cannot tolerate it or who balk at the fertility cost. If a gentler on-ramp can deliver most of the benefit, gene therapy stops being a last resort for the strongest patients and starts looking like an option for more of the people who need it. The authors are careful to call for larger trials, and they are right to. But for seven people, the math of everyday life shifted from dozens of crises to a handful, and it held.
Comments